
CDI tip: COVID-19 and EVALI: Review ICD-10-CM codes implemented mid-year
by Sarah A. Nehring, RHIT, CCS, CCDS
In the IPPS final rule for fiscal year 2022, CMS solidified an April 1 implementation date for ICD-10-CM/PCS code updates (in addition to the annual October 1 update) to fully begin April 1, 2022. CMS recommended a phased-in approach with limited April 1 code updates to start.
This mid-year update will allow earlier capture of diagnoses, procedures, services, and treatments that will benefit ICD-10-CM/PCS reporting, data collection, tracking of clinical outcomes, claims processing, surveillance, research, policy decisions, and data interoperability.
With new COVID-19 codes coming in April 2022, now is a good time to review these updates as well as an ICD-10-CM code that was previously released in an April update: electronic cigarette, or vaping, product use-associated lung injury (EVALI).
April 2022 update
In November, CMS announced the ICD-10-CM/PCS codes that will become effective on April 1, 2022. We’ll have three new ICD-10-CM codes related to COVID vaccination status:
- Z28.310, unvaccinated for COVID-19
- Z28.311, partially vaccinated for COVID-19
- Z28.39, other under-immunization status
All three ICD-10-CM codes are non-comorbid conditions and will not impact the MS-DRG.
In addition, we’ll have seven new ICD-10-PCS codes related to COVID-19 vaccine and fostamatinib treatment:
- XW013V7, Introduction of COVID-19 vaccine dose 3 into subcutaneous tissue, percutaneous approach, new technology group
- XW013W7, Introduction of COVID-19 vaccine booster into subcutaneous tissue, percutaneous approach, new technology group 7
- XW023V7, Introduction of COVID-19 vaccine dose 3 into muscle, percutaneous approach, new technology group 7
- XW023W7, Introduction of COVID-19 vaccine booster into muscle, percutaneous approach, new technology group 7
- XW0DXR7, Introduction of fostamatinib into mouth and pharynx, external approach, new technology group 7
- XW0G7R7, Introduction of fostamatinib into upper GI, via natural or artificial opening, new technology group 7
- XW0H7R7, Introduction of fostamatinib into lower GI, via natural or artificial opening, new technology group 7
All of these new ICD-10-PCS codes have a non-OR designation and will not impact the MS-DRG.
Fostamatinib is a medication used to treat chronic immune thrombocytopenia-ITP. However, studies have been done to evaluate the effectiveness of fostamatinib in treatment of patients hospitalized with COVID-19.
According to the September 14, 2021, ICD-10-CM Coordination and Maintenance Committee Meeting agenda, “a request for emergency use authorization (EUA) is under review by the U.S. Food and Drug Administration (FDA) for the treatment of hospitalized COVID-19 patients. If approved by the FDA under its COVID-19 EUA, fostamatinib will become eligible for the new COVID-19 treatment add-on payment.”
EVALI
Because most of the mid-year updates so far have been COVID-19-related, it’s easy to view them as a direct result of the pandemic. However, one of the very first codes CMS proposed and implemented in an April update was for EVALI. ICD-10-CM code U07.0, Vaping-related disorder, became effective on April 1, 2020, at the same time as ICD-10-CM code U07.1, COVID-19.
There was a time not that long ago that EVALI reporting was a hot topic in coding and documentation articles, forums, and water cooler discussions. The first case of EVALI was reported to the Centers for Disease Control and Prevention in August 2019, and the number of cases peaked in September 2019. Approximately 2,800 EVALI cases and 68 deaths had been reported as of February 18, 2020.
Due to the emergence of COVID-19 and the decline in incidence of EVALI cases (possibly due to the banning of certain e-vaping products), EVALI fell out of the limelight. So much so that when recently asked by a provider about EVALI reporting, I had to refresh my memory by checking the guidelines.
EVALI may have moved backstage when COVID-19 entered the scene, but it isn’t gone for good—and it may be more dangerous than ever. A population-based study published in August of 2020 suggests that young adult patients who vape are at an increased risk of COVID-19 infection.
Let’s revisit how it should be reported in ICD-10-CM.
If a provider documents an e-cigarette or vaping related condition, code U07.0 should be assigned. If the vaping-related condition is the reason for admission, code U07.0 should be sequenced as principal diagnosis.
According to the ICD-10-CM Official Guidelines for Coding and Reporting, additional codes should be assigned for any documented manifestations of EVALI. Complications of EVALI include acute respiratory distress syndrome (ARDS), acute respiratory failure, acute pneumonitis, organizing pneumonia, and/or the need for mechanical ventilation.
When U07.0 is sequenced as principal diagnosis, and no procedure with OR designation is assigned, the case will group to MS-DRGs 205 and 206 (Other respiratory system diagnosis with MCC and without MCC). Only an MCC will impact the MS-DRG. Coding mechanical ventilation can impact the MS-DRG, as well.
The table below shows the impact that some common manifestations (secondary diagnoses) and mechanical ventilation procedure codes can have on the MS-DRG when U07.0 is sequenced as principal diagnosis:
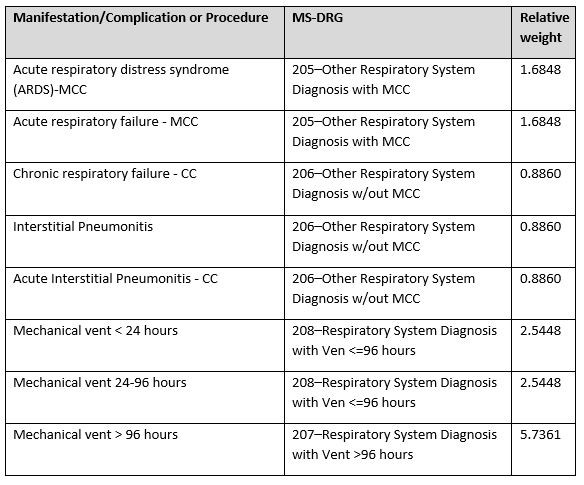
ICD-10-CM code U07.0 as a secondary diagnosis is not CC or MCC, so it will not impact the MS-DRG, but documented manifestations might. It so important that the condition be coded thoroughly.
According to the ICD-10-CM Official Guidelines for Coding and Reporting:
Associated respiratory signs and symptoms due to vaping, such as cough, shortness of breath, etc., are not coded separately, when a definitive diagnosis has been established. However, it would be appropriate to code separately any gastrointestinal symptoms, such as diarrhea and abdominal pain.
Case examples
Example 1: An 18-year-old female presents with a cough, shortness of breath and chest pain. Her O2 saturations are in the low to mid 80s. She’s placed on oxygen. She’s febrile and a check x-ray shows lung opacities concerning for pneumonia/pneumonitis. Her COVID-19 test is negative. She’s started on IV antibiotics for possible community acquired pneumonia (CAP), but after two days there is little to no improvement in her symptoms. A CT of chest reveals no improvement in opacities. She reveals that she’s recently been vaping cannabis. IV antibiotics are discontinued, and she’s started on corticosteroid treatment with improvement in symptoms. The final diagnosis is acute hypoxic respiratory failure from suspected pneumonitis from cannabis vaping, CAP ruled out.
ICD-10-CM code assignment for this case:
- Principal diagnosis
- U07.0, vaping-related lung injury
- Secondary diagnoses
- J96.01, acute hypoxic respiratory failure
- J69. 1, pneumonitis due to inhalation of oils and essences
- MS-DRG
- 205, Other Respiratory System Diagnosis with MCC (RW 1.6848)
Example 2: A 25-year-old male presents with shortness of breath and chest tightness. His O2 saturations are 84%, and he’s placed on oxygen. The patient has a three-year history of vaping cannabis but has been trying to cut down recently. A check x-ray and CT of the lungs shows multi-lobar ground glass opacities with evidence of possible organizing pneumonia. A COVID-19 test is positive, and the patient is admitted. Provider documentation during the admission indicates acute hypoxic respiratory failure due to COVID-19 pneumonia and possible vaping-related lung injury. At the time of discharge, the attending provider documents COVID-19 pneumonia and states in the hospital course summary that vaping-related lung injury cannot be ruled out as a contributing factor.
ICD-10-CM code assignment for this case:
- Principal diagnosis
- U07.1, COVID 19
- Secondary diagnoses
- J12.82, pneumonia due to coronavirus disease 2019
- J96.01, acute hypoxic respiratory failure
- U07.0, vaping-related lung injury
- MS-DRG:
- 177, Respiratory Infection and Inflammation with MCC (RW 1.8491)
Conclusion
The emergence of EVALI and COVID-19 have changed the pace of change we can expect in future. As we embrace the new, we must be careful not lose sight of all that has come before it.
References and further reading
E-cigarettes and vaping-related disease. New England Journal of Medicine. (n.d.). Retrieved December 8, 2021, from https://www.nejm.org/vaping.
The EVALI outbreak and vaping in the COVID-19 era. The Lancet Respiratory Medicine. (2020, August 14). Retrieved December 1, 2021, from https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(20)30360-X/fulltext.
Editor’s note: This article was originally published by ACDIS’ sister publication, JustCoding. Nehring is the inpatient lead coding educator at a large teaching hospital in central Illinois. Contact her at nehrings4@gmail.com. Opinions expressed do not necessarily reflect those of HCPro, ACDIS, or any of its subsidiaries. For questions contact editor Amanda Norris at anorris@hcpro.com.